Contribution 01
CRCD — a window into real robotic surgery
To teach a robot, you first need examples. The Comprehensive Robotic Cholecystectomy Dataset (CRCD)
is one of the most complete public recordings of real robotic gallbladder surgeries ever released — think of
it as a richly annotated “textbook” of how experts actually operate.
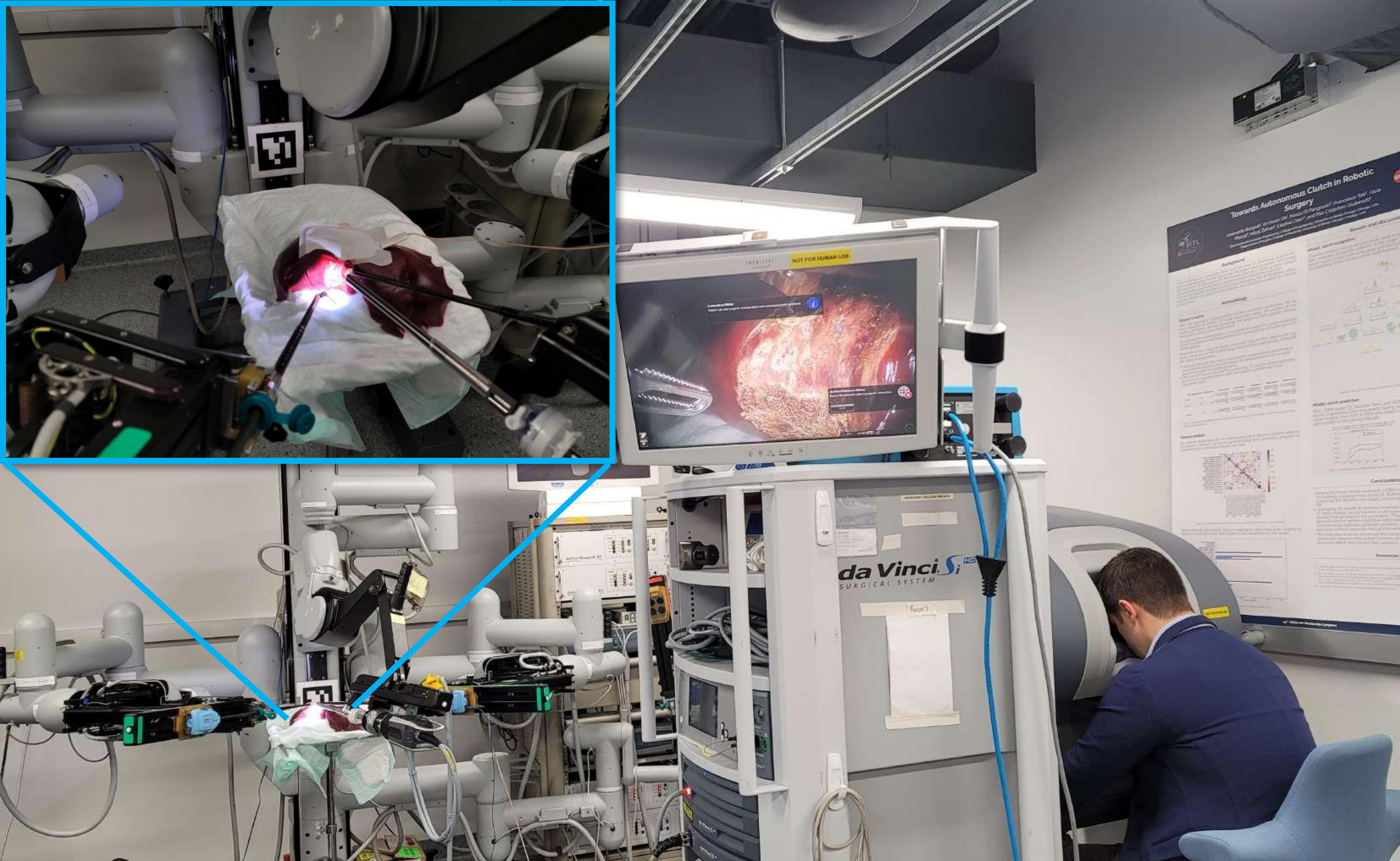
It was recorded during ex vivo procedures on porcine (pig) livers and brings together, perfectly
time-synchronized, every signal a learning system could want:
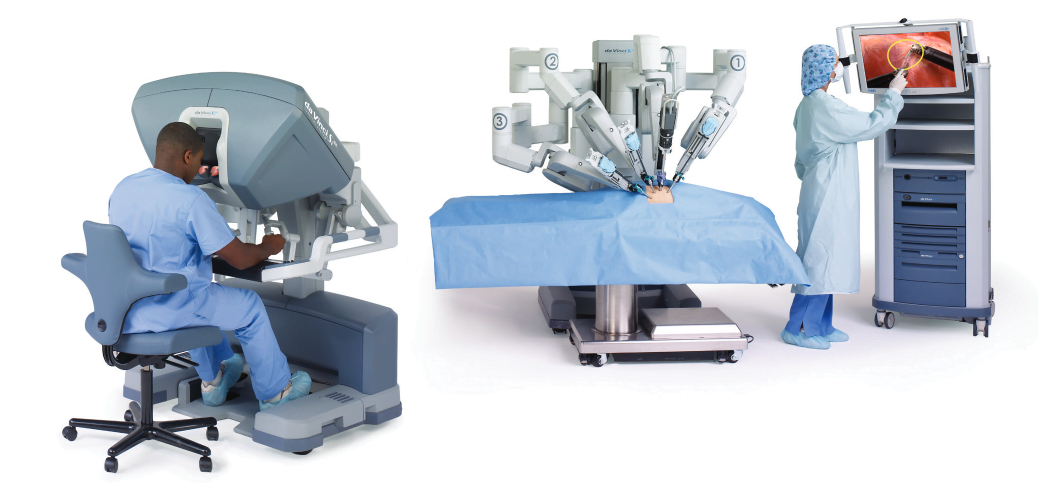
- Stereo endoscopic video — the robot's 3D view inside the body
- Full robot & console kinematics — exactly how every arm and the surgeon's hands moved
- Foot-pedal signals — when the surgeon delivered cutting/sealing energy (rarely shared publicly)
- Dense annotations — tissue segmentation and instrument keypoints
755,000+ stereo frames
7 surgeons, rated by experience
Multimodal & synchronized
CC-BY-4.0
Why it matters: existing datasets were missing something — kinematics, the surgeon's
hand motion, pedal signals, or dense labels on a real procedure. CRCD brings them together, so
researchers worldwide can train and fairly compare perception, control, and learning models.